Every Emergency Manager familiar with the capability of EMIS or CIMS systems talks about the need to have 'Dashboards' - display views showing critical information that are often shaded or coloured to highlight particular values based on priority, time due, alert level etc.
Unfortunately as much as everyone thinks they are a good thing (and the answer to all their briefing problems), no-one can really agree on what should actually be in a dashboard. Over the last year or so I've learnt that whilst most database EMIS systems can be built to record and display whatever their administrator or project manager can think of, the real challenge is in identifying data of worth that needs to be displayed.
Some of the NZ Health Emergency Managers may remember a WebEOC board that was used during the WebEOC trial in Ex Cruickshank May 2007. That board was based on the second page of the national health sitrep and allowed a District Health Board to report on bed availability, staff shortages, infrastructure damage, system status and utility failure.
Whilst this was turned into a great looking WebEOC board (a consolidated series of screenshots for 'Shortland St' Hospital is shown below) it underlined the fundamental difficulty in designing effective dashboards - that is how do you usefully record dashboard information such as fire, water damage, power outages or staff shortages for multi-sited, mulit-building, multi-department sites like a modern healthcare facility?
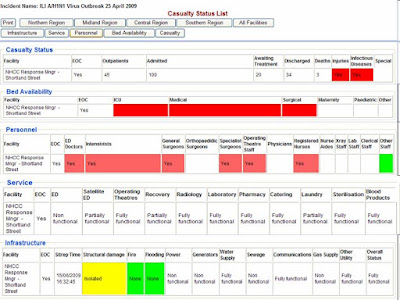
For example the paper based form had the ability to record as 'Functioning' 'Partially Functioning' and 'Not Functioning' for utility and service status that was subdivided into Electricity, Gas, Potable Water, Steam, Sewerage etc. Whilst these three values are easily added to a WebEOC form as a drop down field, and can be shaded in the display view green, orange and red the trouble is it does not really tell you what you need to know.
If Power is 'Partially Functioning' what does that actually mean on a multi-building hospital site, how does the partial power outage impact on the ability to receive casualties? What if it is in the Emergency Department - then there may still be options around field triage or generators but if it is in other departments, such as imaging or ICU the effects may be much greater.
Bed availability is another area that on first glance looks easy but is notoriously difficult to record within a dashboard. Intensive Care Unit capacity is not just the physical bed but also require trained staff, equipment such as ventilators and support systems. Furthermore clinical staff are excellent at actually freeing up capacity when it is required but all of this is dependent on capacity of other departments and wards and is not something that can easily be entered.
Some of the most successful dashboards in this area have been developed in jurisdictions that are linked to business as usual systems, especially Patient Management Systems. For example EM Systems provide a PMS that is used in about a third of US hospitals and is constantly updated on patient location, bed availability and staffing.
In the event of a hospital activating their Emergency Plan this data is immediately available to WebEOC via a special Application Program Interface. The advantages of this are obvious, clinical and clerical staff can get on with responding to the influx of casualties whilst the Emergency Operations Centre will have access to real time data right from the start of the incident.
The design of the NZ Health EMIS is such that it is intended to also support local incidents and not simply to be used in regional or national events. Over the last couple of weeks we've developed a number of APIs for this instance of WebEOC and going forward there is no reason why any NZ Health agency cannot develop APIs between their own business as usual systems and WebEOC.
With the Influenza response ongoing for the forseeable future I'm currently working on some options to host the next EMIS Reference Group meeting and another 'Board Building Boot Camp' to train some additional adminsitrators.
In the event of a hospital activating their Emergency Plan this data is immediately available to WebEOC via a special Application Program Interface. The advantages of this are obvious, clinical and clerical staff can get on with responding to the influx of casualties whilst the Emergency Operations Centre will have access to real time data right from the start of the incident.
The design of the NZ Health EMIS is such that it is intended to also support local incidents and not simply to be used in regional or national events. Over the last couple of weeks we've developed a number of APIs for this instance of WebEOC and going forward there is no reason why any NZ Health agency cannot develop APIs between their own business as usual systems and WebEOC.
With the Influenza response ongoing for the forseeable future I'm currently working on some options to host the next EMIS Reference Group meeting and another 'Board Building Boot Camp' to train some additional adminsitrators.


No comments:
Post a Comment